
Restoring Function. Embracing Life.
SLAP Lesion Repair Specialist in Singapore
Dr Bryan Wang
Consultant Orthopaedic Surgeon
Trusted Orthopaedic Surgeon | Fellowship-trained in Canada | With over 20-years of experience
SLAP Lesion Repair
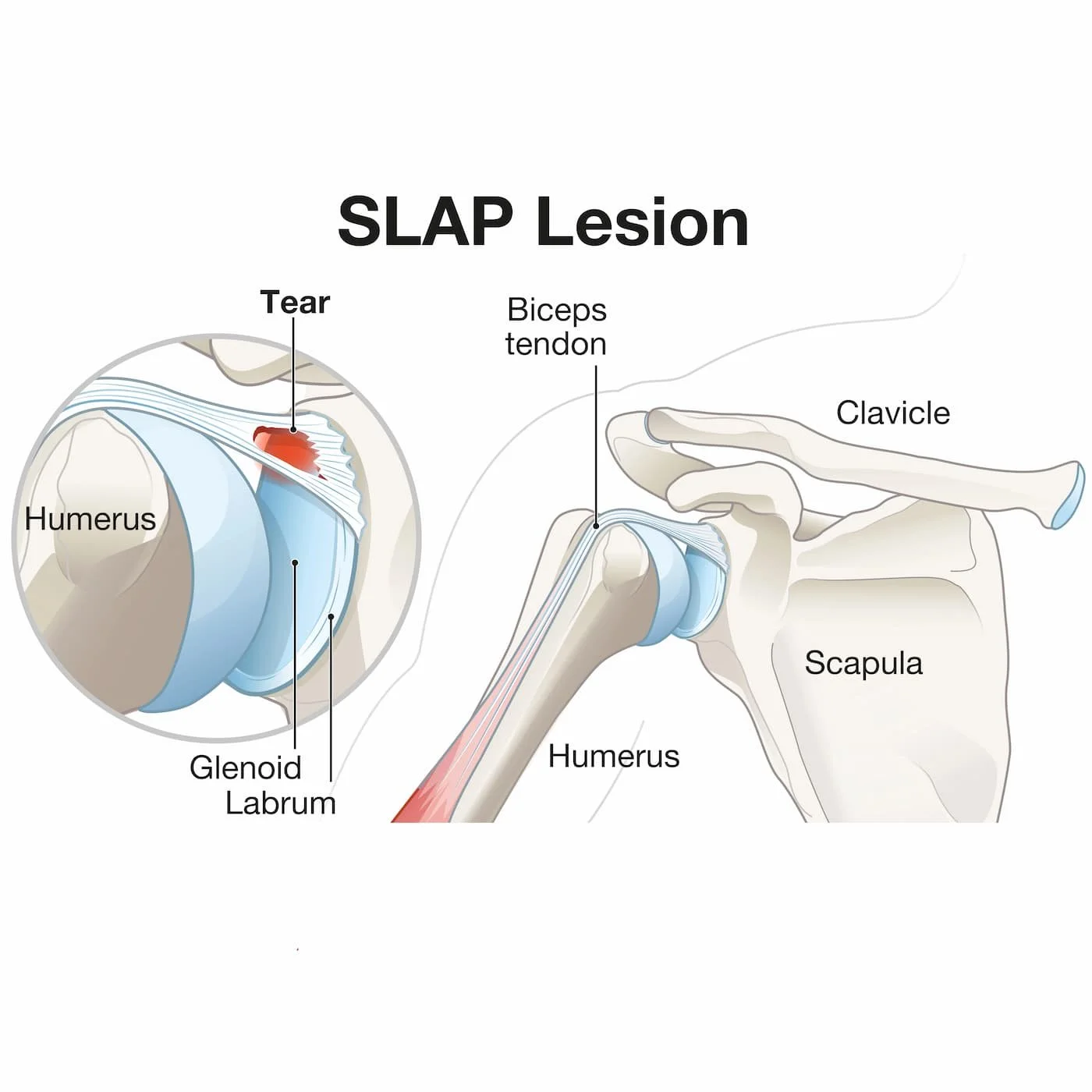
A Superior Labral Anterior Posterior (SLAP) Lesion is a tear of the top part of the glenoid labrum where the biceps tendon anchors. It commonly occurs in a fall on an outstretched hand (FOOSH) injury or sometimes with repetitive overhead sports. It causes deep shoulder pain, clicking, and loss of trust in the shoulder. It is diagnosed via specific physical tests and MRI arthrogram. Treatment ranges from targeted physiotherapy to arthroscopic repair or biceps tenodesis depending on age, sport, and associated instability.

What is a SLAP tear?
The glenoid labrum is a tough rim of cartilage that deepens the shoulder socket and anchors key ligaments and part of the biceps tendon. When it tears, the “socket” loses its grip and depth making the joint feel loose or unstable—especially during throwing, swimming, pressing, or contact sports. Shoulder Instability can be a full dislocation (ball comes out completely) or a subluxation (partial slip that “clunks” back).
Symptoms At a Glance
Patients with a SLAP tear may present with the following symptoms:
Deep shoulder pain that may be intermittent and increases with overhead activity or lifting
Painful clicking or a sense of giving way
Pain with throwing/serving or during push-ups/presses
Weakness or loss of power of the affected arm
Fatigue with repetitive use of the shoulder
Night pain or discomfort lying on the affected side
When Do I Need to See a Shoulder Specialist?
You might need to consult a shoulder specialist or the Accident and Emergency Department if you experience the following:
There is a visible deformity after a first-time dislocation
There is numbness, pins-and-needles, or weakness of the arm after a traumatic fall or an injury
Severe pain with inability to move the arm (possible fracture/dislocation)
SLAP Lesion Treatment
How do Diagnose a SLAP Lesion?
The symptoms of a SLAP lesion often overlap with other shoulder conditions like Bankart Lesion or Rotator Cuff Injury. Hence the diagnosis relies on a combination of clinical evaluation, imaging, and sometimes arthroscopy. The goal is to confirm labral involvement and identify the tear’s location and severity.
Specialist Physical Examination
Clinical history
sensations of painful clicking and/or popping with shoulder movement
loss of glenohumeral internal rotation range of motion
pain with overhead motions
loss of scapular stabiliser/ rotator cuff muscle strength and endurance
inability to lie on the affected shoulder
Labral provocation tests such as:
O’Brien’s Test
Apprehension Test
Compression Rotation Test etc
Imaging
X-rays to screen for bony injuries (e.g., Hill–Sachs, bony Bankart)
MRI or MRI arthrogram to visualise the superior labrum and biceps anchor
CT Arthrogram if MRI is contraindicated
What are my Treatment Options for a SLAP Tear?
Most patients start with non-surgical care; surgery is considered when symptoms persist, or performance goals require it.
SLAP Tear Conservative Treatment (non-surgical)
Cessation of provocative overhead positions/ activities initially.
Physiotherapy/rehabilitation: scapular control, rotator-cuff endurance, kinetic chain and proprioception.
Short course of analgesia/ selective image-guided injections can help pain control during rehab.
SLAP Tear Surgical Treatment:
Arthroscopic SLAP repair: It is indicated in younger athletes who need the biceps anchor intact for overhead activities. Procedure includes reattachment of the superior labrum to the glenoid using suture anchors.
Biceps tenodesis: It is commonly done in adults (> 35 y.o) where there may be degenerative labral tears or a failed SLAP repair. Procedure includes release of the diseased biceps anchor and re-fixing the tendon on the humerus.
Biceps Tenotomy: Indicated in elderly patients with extensive pain or those with low demand of the shoulder. The biceps tendon is simply released from the labrum and this may have a slight cosmetic deformity.

SLAP Lesion Rehabilitation
Post operative SLAP Lesion Rehabilitation following a SLAP repair depends on the surgical procedure done and any other associated pathology. The general guideline for SLAP Lesion Rehabilitation is as follows:
1. Initial Phase (~ 0-3 weeks)
Rest the shoulder; apply ice; avoid overhead or throwing movements
Use supportive taping or sling (if advised by doctor)
Gentle range-of-motion (ROM) exercises for elbow, wrist, and hand
Isometric shoulder exercises to maintain muscle activation
2. Intermediate Phase (~ 4-8 weeks)
Gradual passive and active-assisted ROM exercises for flexion, abduction, and rotation
Scapular stabilisation training, Neuromuscular control drills to re-educate shoulder joint stability
Progressive strengthening of rotator cuff and periscapular muscles
Postural retraining to reduce anterior shoulder strain
3. Advanced Phase (~ 9-16 weeks)
Gradual resistance exercises of the shoulder girdle muscles
Dynamic strengthening through closed-chain and proprioceptive exercises
Gradual return to overhead and throwing activities under supervision
Emphasis on eccentric control of the biceps and external rotators
Movement retraining to correct faulty throwing or lifting techniques
4. Return to work/ sport (~ 17-24 weeks)
Full, pain-free ROM and shoulder strength ≥90% of the opposite side
Sport-specific drills (e.g., throwing, serving, swimming strokes) under therapist guidance
Maintenance program for rotator cuff and scapular muscles to prevent recurrence
SLAP Lesion vs Bankart Lesion vs Rotator Cuff Injury

Frequently Asked Questions
-
No. A SLAP tear involves the superior labrum/biceps anchor; a rotator cuff tear involves the rotator-cuff tendons. They can coexist but are distinct problems.
-
Through specialist examination (e.g., O’Brien test) and MRI arthrogram when needed to visualise the labrum and biceps anchor.
-
No. Many improve with targeted physiotherapy. Surgery is considered for persistent pain, functional limits, or when sport/work demands require a durable fix.
-
Younger overhead athletes often benefit from SLAP repair; in many adults, biceps tenodesis can provide reliable pain relief and quicker recovery. Decision depends on age, sport, tear type, and associated instability.
-
Those findings point to instability from dislocation. Your surgical management plan may include Bankart repair, Remplissage for an engaging Hill-Sachs, or in cases of glenoid bone loss, a Latarjet procedure.
References
SLAP Lesion: https://www.physio-pedia.com/SLAP_Lesion
SLAP Lesion: https://www.orthobullets.com/shoulder-and-elbow/3053/slap-lesion
Beacon Orthopaedics – About Dr Bryan Wang https://www.beaconortho.com.sg/about-dr-bryan-wang
Medically reviewed by:
Dr Bryan Wang, Consultant Orthopaedic Surgeon, Beacon Orthopaedics (Shoulder & Elbow, Knee & Sports Injuries; fellowship-trained; >20 years’ experience).
Last reviewed: October 2025.
Educational content only; not a substitute for personalised medical advice. Book an appointment at Beacon Orthopaedics to discuss your diagnosis and treatment options
Why choose Beacon Orthopaedics?
Leading Shoulder & Sports Injury Specialist
Your care is led by Dr Bryan Wang, a fellowship-trained Shoulder & Elbow and Sports Injury specialist (Pan Am Clinic, Canada) and former Senior Consultant at Changi General Hospital. He also teaches at NUS, NTU, and Duke-NUS, and is a member of AAOS, ISAKOS, and the Canadian Shoulder & Elbow Society.
Athlete-Centred Treatment
From professional athletes to weekend warriors, Dr Wang tailors’ treatment plans to ensure a safe, effective return to sport. His evidence-based approach helps restore shoulder strength and stability after a SLAP tear.
One-Stop Clinic
Enjoy comprehensive care under one roof — including same-week imaging (X-ray, MRI), on-site or partner physiotherapy, and clear recovery milestones for a seamless return to work or sport.
Minimally Invasive Approach
Dr Wang believes in a keyhole-first (arthroscopic) approach whenever suitable. Using advanced arthroscopic shoulder repair techniques, he aims for smaller incisions, less pain, and faster recovery — helping patients return to their active lifestyles sooner.
Ready To Get Confident with Your Shoulder Again?
If you’re experiencing recurrent shoulder dislocations, pain after overhead activity, or suspect a labral tear, book an appointment with Beacon Orthopaedics, Singapore.
Early, accurate diagnosis and a structured plan can get you back to work, sport, and daily life with confidence.
